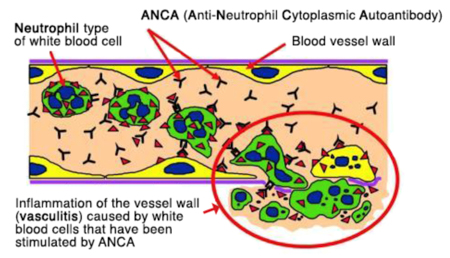
Vasculitis is the inflammation of vascular structure by the presence inflammatory leukocytes in vessel wall leading to damage of mural structure and resultant downstream tissue ischemia and necrosis. Anti-neutrophil cytoplasmic antibodies (ANCAs) are a group of autoantibodies, mainly of the IgG type, against antigens in the cytoplasm of neutrophil granulocytes and monocytes. There are two main kinds of ANCA. Each targets a specific protein inside white blood cells –
- pANCA, which targets a protein called MPO (myeloperoxidase)
- cANCA, which targets a protein called PR3 (proteinase 3)
Small-vessel vasculitis are mainly relates to ANCA. They may be further classified as –
- ANCA associated – Microscopic polyangiitis, Wegener’s granulomatosis, Churg-Strauss syndrome, and Drug-induced vasculitis
- Non-ANCA associated vasculitis
Interpretation
Monitoring the titers of ANCAs are useful in monitoring the clinical course of diseases
- Positive results for c-ANCA are mostly consistent with granulomatosis with polyangiitis (GPA or Wegener granulomatosis).
- Positive results with p-ANCA mostly occur in microscopic polyangiitis (MPA) and eosinophilic granulomatosis with polyangiitis (EGPA or Churg-Strauss syndrome).
Mnemonic – We Can (Wegner for c-ANCA), My Pan (Microscopic polyangiitis for p-ANCA)
Key point
- The ANCA associated vasculitides (AAV) are rare multisystem autoimmune diseases
- More common in older people and in men
- For induction treatment Cyclophosphamide or Rituximab and Glucocorticoids are used
- AAV should be considered to be a chronic disease needing long term immunosuppressive therapy
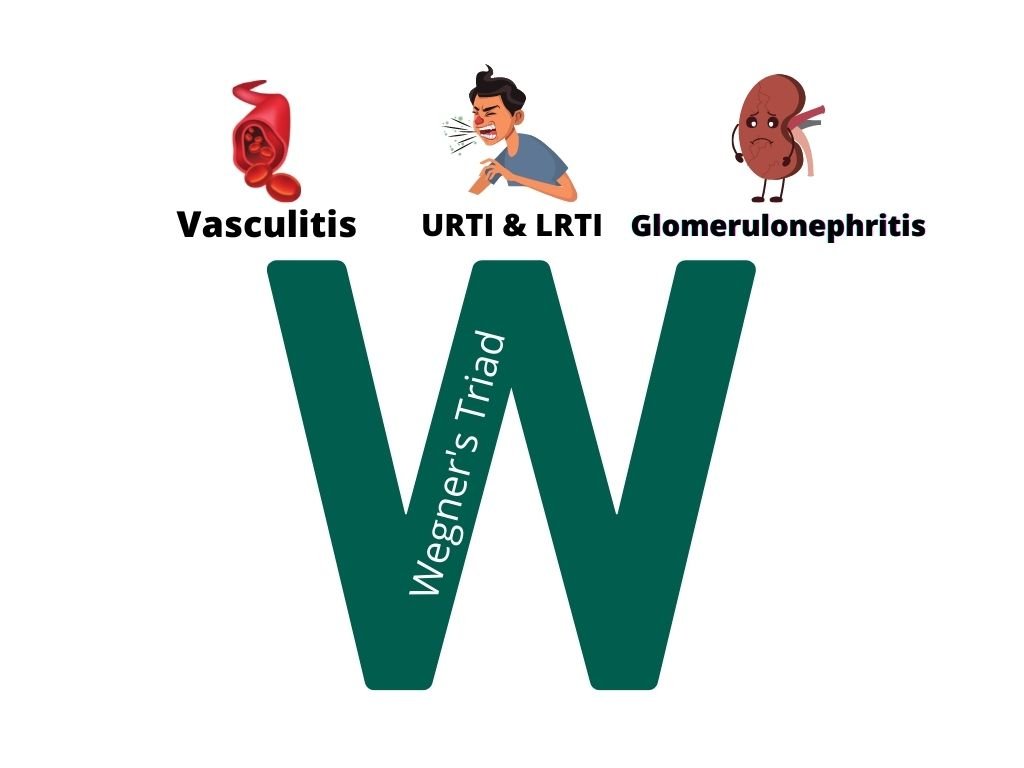
Wegener Granulomatosis
Also called as Granulomatosis with Polyangiitis (GPA). Granulomatosis with polyangiitis commonly involves a triad of –
- Upper respiratory tract (sinusitis, crusting rhinitis, saddle nose deformity, otitis media, mastoiditis, hearing loss), and lower respiratory tract (lung nodules, alveolar hemorrhage) involvement
- Systemic vasculitis
- Kidney involvement (glomerulonephritis)

MPA(Microscopic polyangiitis)
Only 70% of cases of MPA have ANCA at the time of diagnosis, and most of the cases of limited MPA do not have ANCA at all
Clinical Presentation –
- Insidious onset fever, arthralgia, weight loss, urinary abnormalities, cough with or without hemoptysis
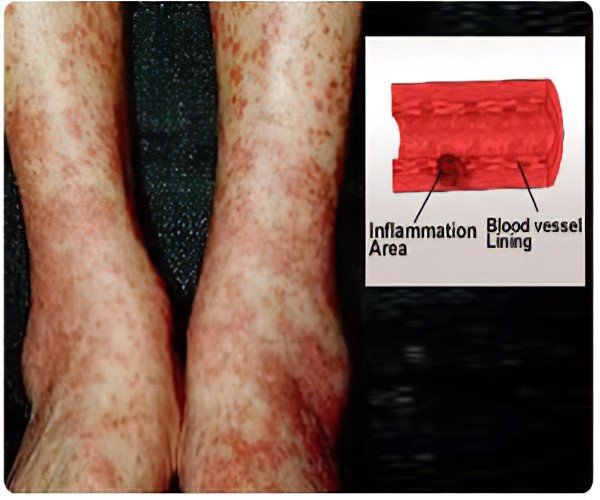
- Skin findings consistent with palpable purpura, or non-specific neurological complaints
- Some patients may present with acute onset of fulminant disease with frank hemoptysis, hematuria, or even renal failure
- Renal manifestations are most common, and up to 80% to 100% of individuals have some form of glomerulonephritis at onset or with disease progression.
- The most common manifestation is a “pauci-immune” form of rapidly progressive glomerulonephritis (RPGN). Clinical presentation may vary from asymptomatic hematuria, sub-nephrotic proteinuria, a rise in serum creatinine, or overt renal failure
Churg Strauss Syndrome
Also called as Eosinophilic Granulomatosis with Polyangiitis (EGPA). Regardless of age, adult and childhood EGPA both present with highly elevated IgE and eosinophil levels. About 40% of adults have a positive ANCA, while 25% of children are seropositive.


[Thin section CT scan at carina shows multifocal patchy ground-glass opacity around the patchy consolidation showing halo sign (arrows}]
 [Right perihilar consolidation, Focal opacity mainly in Right upper zone]
[Right perihilar consolidation, Focal opacity mainly in Right upper zone]
The clinical course is characterized by 3 phases, which do not necessarily always present in every patient. They may even overlap in the natural history of an individual’s disease.
- In the initial prodromal phase, nonspecific symptoms of malaise, fever, migrating polyarthralgia, and weight loss are common, along with a severe adult-onset form of asthma that is refractory to conventional treatment
- The second phase is characterized by eosinophilic infiltrates in end organs along with peripheral eosinophilia. Patchy peripheral nodular pulmonary infiltrates, eosinophilic gastroenteritis, serosal effusion, are common.
- An onset of vasculitis characterizes the third phase, and it may take anywhere between 3 to 9 years since the onset of asthma. Neurological symptoms are a hallmark of this phase.

Drug Induced Vasculitis
The most common drugs associated with vasculitis are Propylthiouracil, hydralazine, minocycline, allopurinol, D-penicillamine, sulfasalazine, penicillin, cephalosporins and several immunomodulating agents




Thank you for your preparing latest books tor health students.
excellent crisp presentation