DERMATOMYOSITIS
- Dermatomyositis is an idiopathic inflammatory myopathy with proximal weakness and characteristic cutaneous findings.
- It has biphasic peaks. Seen in children aged 7-15 years and adults aged 30-50 years.
- It is more predominant in females.
PATHOPHYSIOLOGY
- Dermatomyositis is mediated by Type 1 interferon cytokine family (IFN alpha, IFN beta)
- Classic antibodies associated are anti-Mi-2 against helicase and anti-Jo-1 (antisynthetase antibody).
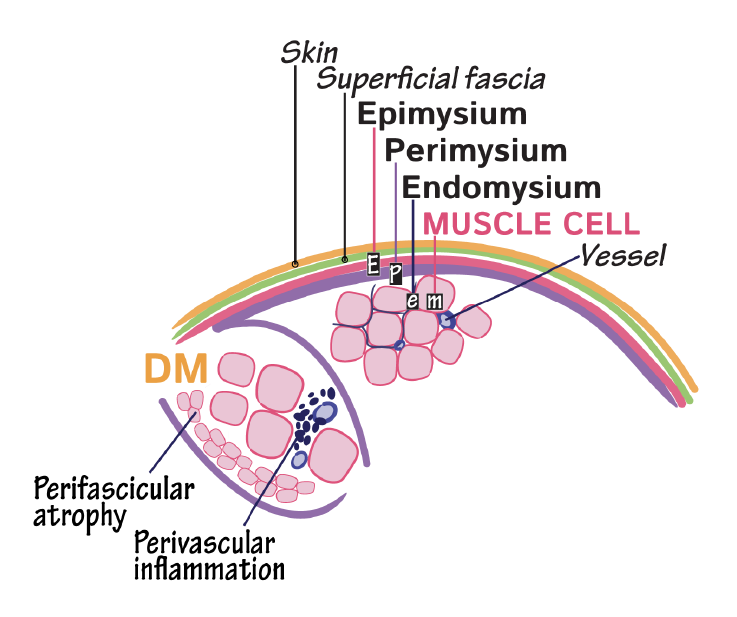
- Muscle pathology involves injury to muscle capillaries and perifascicular atrophy (injury to muscle fibers at the end of muscle fascicles).
- Skin pathology involves injury to the basal layer of keratinocytes.
SIGNS AND SYMPTOMS:
Skin
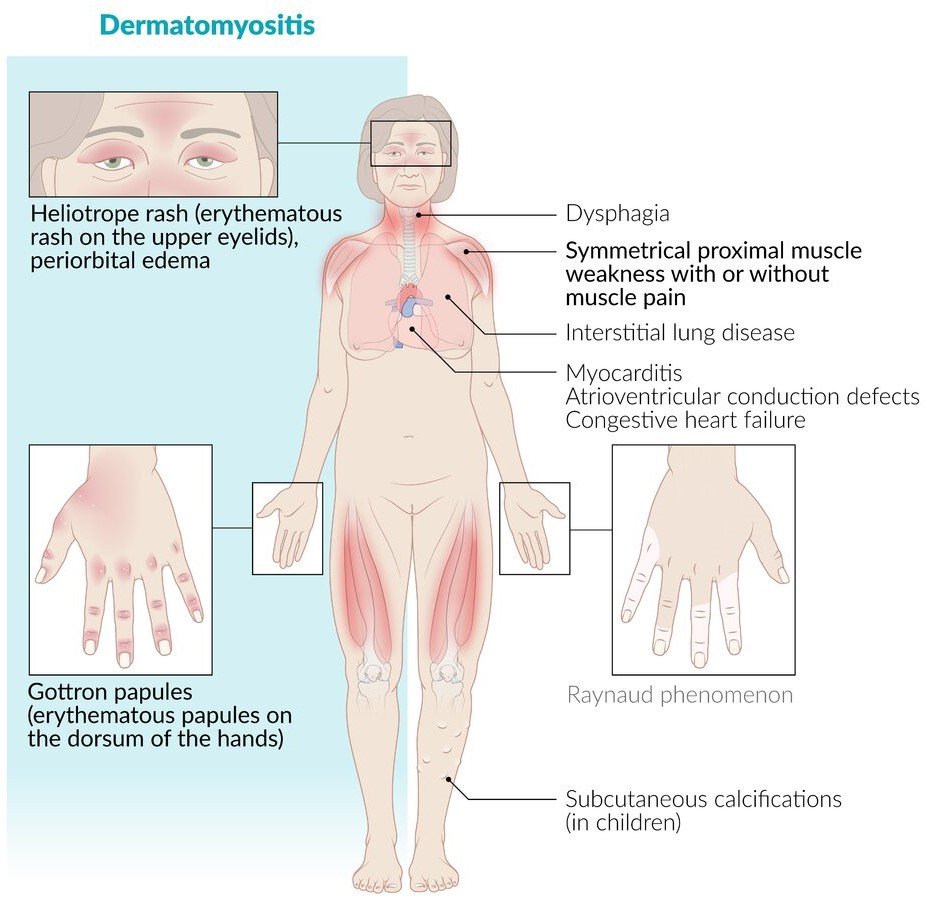
- Gottron’s sign/papules: Violaceous lesions that can be flat (Gottron sign) or raised (Gottron papules) over dorsal metacarpophalangeal and interphalangeal joints of the hands, elbows, knees.
- Heliotrope rash: Violaceous periorbital macular erythema with or without edema.
- Butterfly-shaped, malar erythematous rash (note that malar refers to its site: the cheek and butterfly refers to its shape).
- It crosses the nasolabial folds because this distinguishes it from the malar rash of systemic lupus erythematosus, which spares the nasolabial folds.
- Erythema and poikiloderma on the photo exposed areas –
- On the Chest (V SIGN)
- On the Shoulder, Neck, Back (THE SHAWL SIGN)
- Calcinosis cutis, which is aberrant calcium depositions in the skin and subcutaneous tissues, which cause yellowish or white dermal lesions and stiffening with finger joint immobility.

Muscle
- Symmetric proximal muscle weakness (muscle weakness when combing hair, reaching for objects overhead, rising from a seated position, climbing stairs).
- Extensor muscles are more often affected than the flexor muscles.
Systemic Manifestations
- Dysphagia, GERD
- Myocarditis
- Interstitial lung disease
- Dysphonia
- Subcutaneous calcifications (Calcinosis cutis)
- Flexion contracture of the ankles (tip toe gait in children)
- Malignancies are common in adults, maybe related to cross reacting autoantigens in the muscle and on tumor cells: Most common malignancies are adenocarcinoma (Ovarian, lung, stomach, pancreatic, colorectal).
DIAGNOSTIC CRITERIA
- Diagnostic skin involvement (Gottron’s papule, Heliotrope rash) or diagnostic muscle biopsy findings (Perifascicular atrophy)
OR,
- All of the following –
- Suggestive skin involvement
- Subacute or chronic proximal or distal weakness
- Muscle biopsy showing perimysial or perivascular inflammation without features suggesting another disorder OR skin biopsy showing interface dermatitis along with clinical exclusion of SLE.
LABS:
- Elevated Creatine phosphokinase(CPK) generally 10 times the upper limit or normal but can vary (↑↑CPK)
- Abnormal Aldolase and LDH (↑Aldolase and ↑LDH)
- Antibody studies(anti-Mi 2, anti-Jo-1, anti-MDA5)
- ↑ALT & ↑AST
IMAGING:
- MRI, EMG
BIOPSY:
- Skin biopsy (interface dermatitis)
- Muscle biopsy (Perifascicular atrophy, Perivascular and Perimysial inflammation)
MANAGEMENT
Pharmacological
- Corticosteroids are the first line( typically Prednisolone 1mg/kg/day orally until significant improvement occurs and then gradual taper).
- Second line are Methotrexate, azathioprine, cyclosporine, IVIG.
Non pharmacological
- Avoid sun exposure
- Physical therapy.
Ref: Goldman-Cecil Medicine, Medscape, Uworld, Drawittoknowit, Amboss