Shoulder joint also known as glenohumeral joint. It is multi-axial ball and socket type of synovial joint in which head of humerus articulate with glenoid cavity of scapula. It is flexible joint due to the fact that the socket is very shallow. Hence, allowing more range of movement at articulation.
ARTICULAR SURFACE
It is formed by –
- Large round head of humerus
- Shallow glenoid cavity of the scapula which is deepened slightly by the fibrocartilaginous ring called glenoid labrum.
CAPSULE AND LIGAMENTS
Ligaments help in maintaining the joint. Major contributing ligaments are –
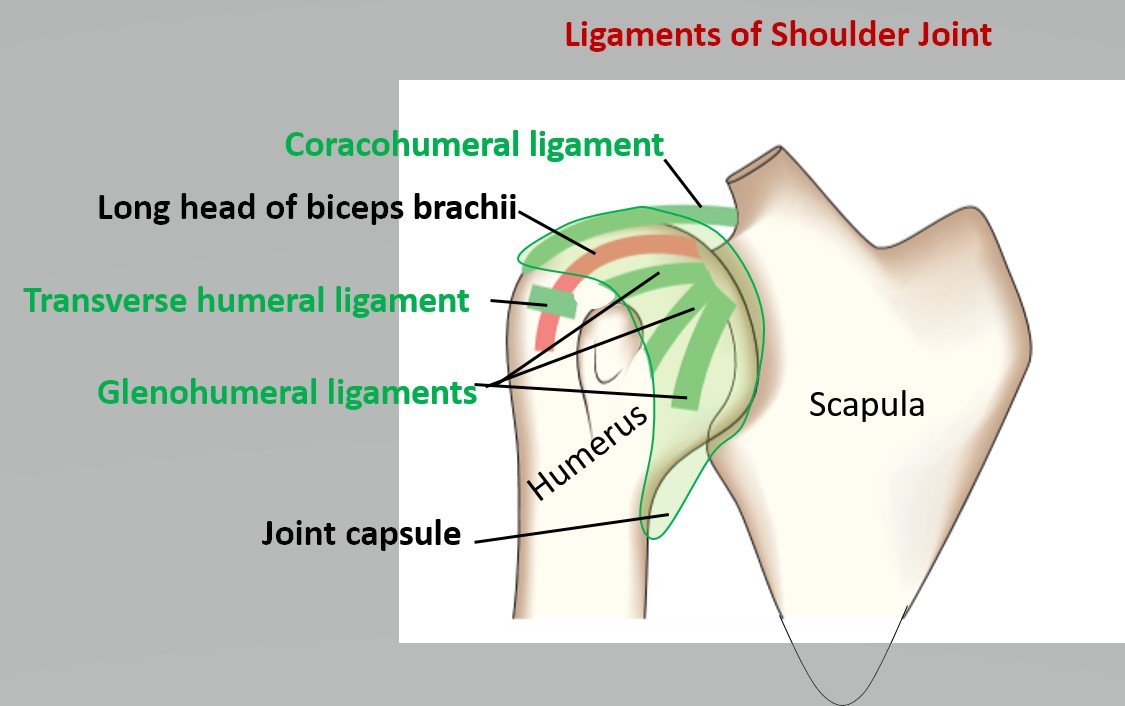
Capsular Ligament (Joint capsule)
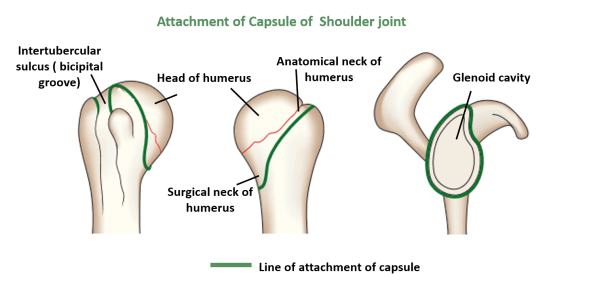
The thin fibrous layer of the joint capsule surrounds the glenohumeral joint. It is attached –
Medially – To the margins of the glenoid cavity beyond the glenoid labrum thus encloses long head of biceps brachii
Laterally – To the anatomical neck of the humerus (except inferiorly where it extends downwards 1.5cm or more on surgical neck of humerus).
Glenohumeral Ligament
Three thickening in anterior part of fibrous capsule to strengthen it Superior, Inferior, and Middle glenohumeral ligament. A defect exists between superior and middle glenohumeral ligament leads to anterior dislocation of shoulder joint.
Coracohumeral Ligament
It is a strong band of fibrous tissue that passes from the base of the coracoid process to the anterior aspect of the greater tubercle of the humerus.
Transverse humeral Ligament
It is a broad fibrous band which bridges bicipital groove between greater and lesser tubercles. This ligament converts the groove into a canal that provides passage to the tendon of long head of biceps surrounded by a synovial sheath.
Some Accessory Ligaments
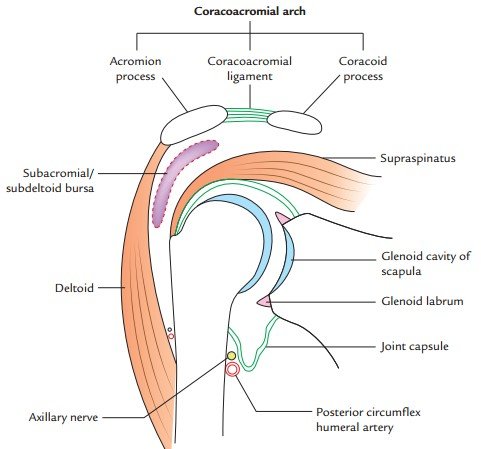
- Coraco acromial ligament – It extends between coracoid and acromion processes. It protects the superior aspect of the joint.
- Coracoacromial arch – It is formed by coracoid process, acromion process, and coracoacromial ligament between them. It prevent superior dislocation of humerus.
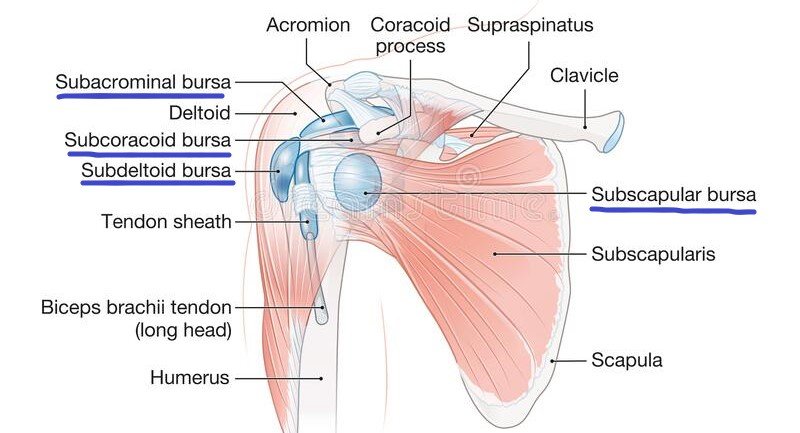
BURSAE OF SHOULDER JOINT
Bursae are fluid filled cavity which reduces friction between two surfaces of the body i.e act as a cushion between them.
Subscapular bursa
It is between subscapularis and neck of scapula which protects tendon from friction against neck.
Sub acromial bursa
It is the largest synovial bursa. It lies between the –
- Coracoacromial ligament and acromion process superiorly
- And supraspinatus tendon and joint capsule inferiorly
This facilitates the movement of supraspinatus tendon.
Infraspinatus bursa
It is present between tendon of infraspinatus and posterolateral aspect of the joint capsule.
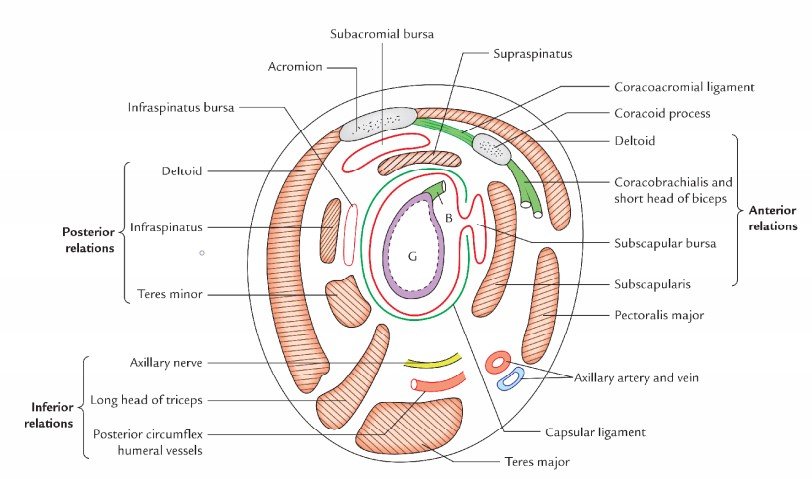
RELATIONS
Above – Coracoacromial arch, Sub acromial bursa, Supraspinatus and Deltoid.
Below – Long head of triceps brachii, Axillary nerves and Posterior circumflex humeral artery
Anteriorly – Subscapularis, Coracobrachialis, Short head of biceps brachii and Deltoid
Posteriorly – Infraspinatus, Teres minor and Deltoid.

STABILITY OF THE JOINT
The fibrous capsule around is too thin and weak to keep humeral head in glenoid cavity, so other structures which help to maintain the stability are –
Muscultendinous cuff/rotator cuff – It is formed by the flattened tendons of the
- Subscapularis anteriorly
- Supraspinatus superiorly
- Infraspinatus and teres minor posteriorly
Glenohumeral ligament – Prevent anterior dislocation.
Coracohumeral ligament – Prevent superior dislocation.
Coracoacromial arch – Prevents the upward dislocation of the head of the humerus.
Glenoid labrum – Deepens the glenoid cavity and prevent skidding of the ball.
Long head of biceps brachii – Prevents the upward dislocation of the head of the humerus.
N.B – Rotator cuff muscles do not support the joint inferiorly
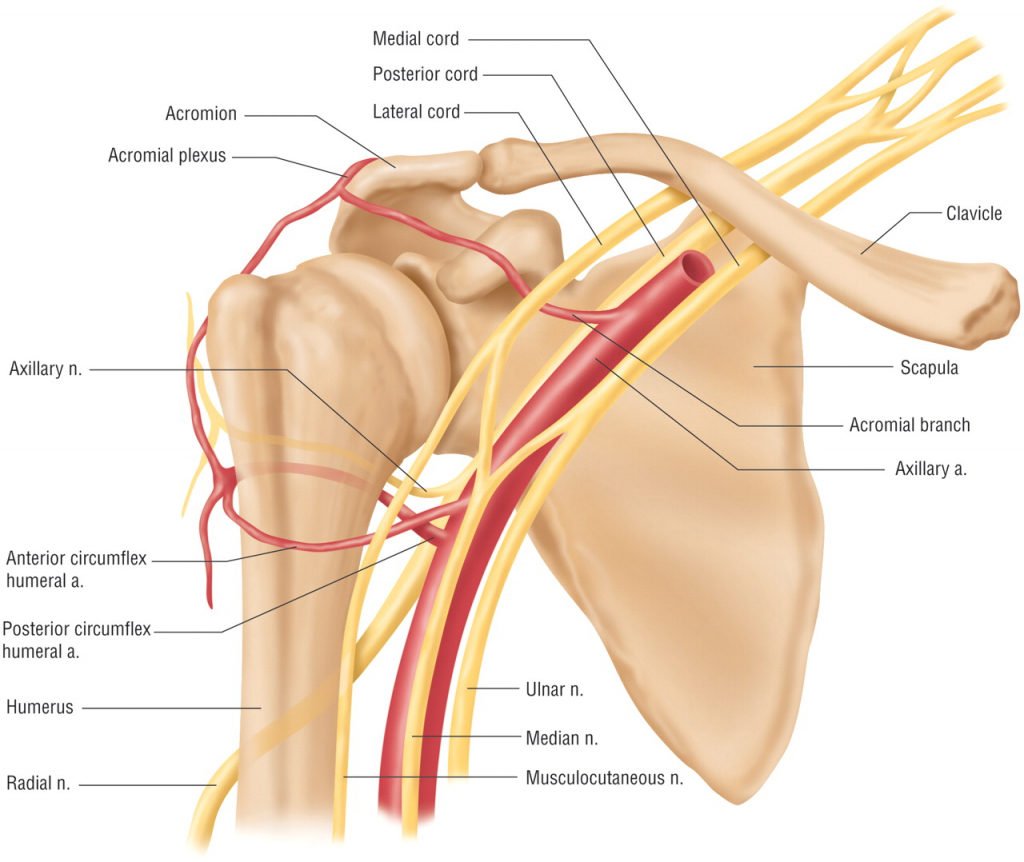
BLOOD SUPPLY
- Anterior and posterior circumflex humeral vessels.
- Suprascapular vessels
- Subscapular vessels
NERVE SUPPLY
- Axillary nerve
- Suprascapular nerve
- Musculocutaneous nerve
MOVEMENTS OF SHOULDER JOINT

ABDUCTION AT SHOULDER JOINT
- The first 15 degree of abduction is done by supraspinatus muscle.
- 15-90 degrees is done by deltoid muscle.
- For overhead abduction, the scapula has to be rotated laterally so that the glenoid cavity gradually faces upwards. This is done by upper fibers of trapezius and serratus anterior muscle. Every 2 degrees of movement at shoulder joint is accompanied by 1 degree of rotation of scapula ( called scapulo-humeral rhythm).
CLINICAL ANATOMY
Shoulder dislocation
Inferior dislocation is common. Glenoid humeral joint is most frequently dislocated large joint. Axillary nerve might get damaged. clinically, it is described as anterior or posterior dislocation indicating whether the humeral head has descended anterior or posterior or to
the infraglenoid tubercle of the scapula and long head of the triceps.
Clinical Features –
- Loss of rounded contour of shoulder
- Prominence of shoulder tip
- Loss of abduction ( between 15-90 degrees ) due to injury of axillary nerve
- Sensory loss over regimental badge area ( skin over lower half of deltoid ) due to injury of axillary nerve


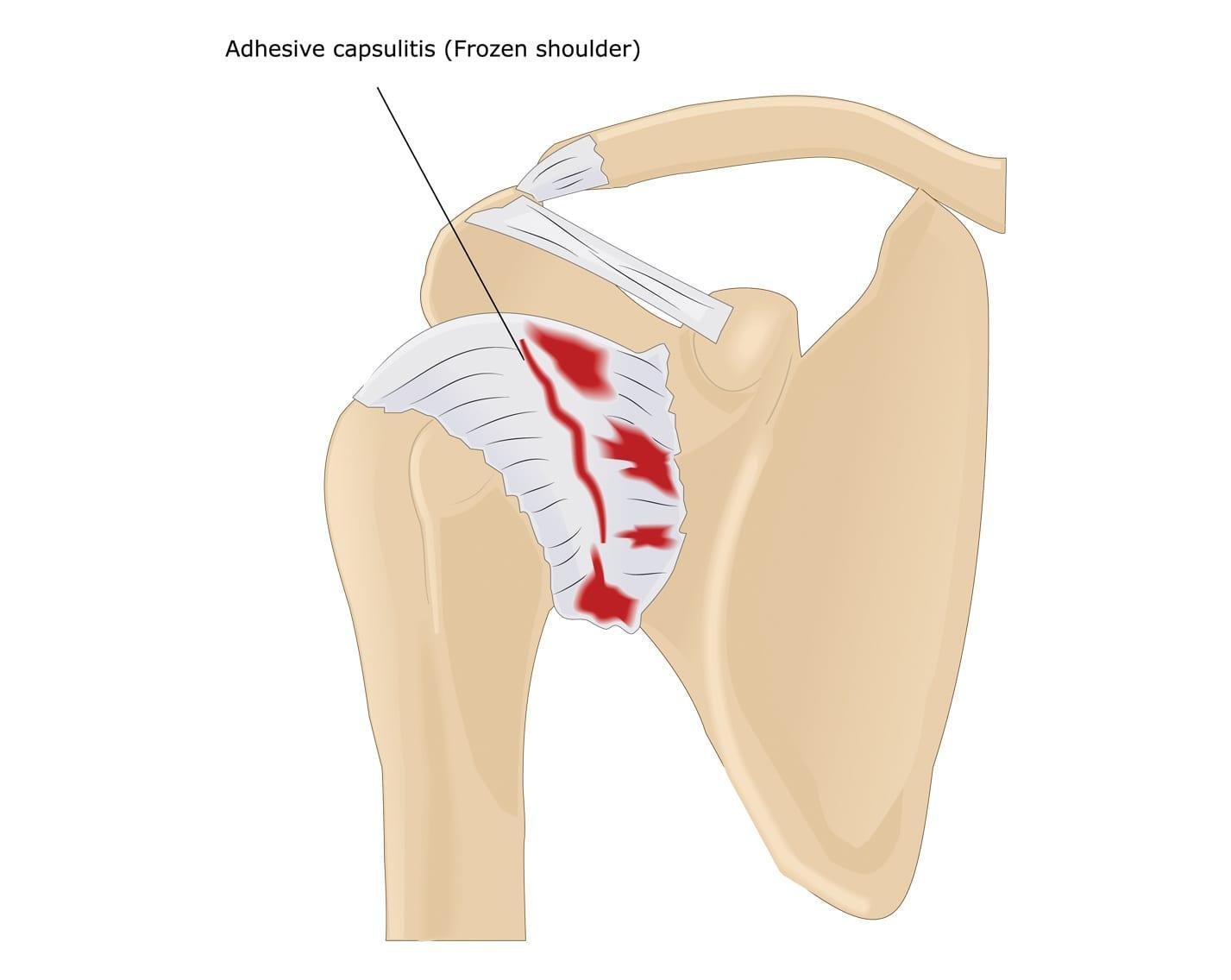
Frozen shoulder
Complete absence of movement at the shoulder joint due to adhesive capsulitis, a disorder in which the capsule and the connective tissue surrounding the shoulder joint becomes inflamed and stiff. Patient recovers in 6-12 month.
Painful arc syndrome
It is also known as impingement syndrome characterized by chronic thickening in the supraspinatus tendon. Pain is experienced between 60°-120° of abduction due to impingement of tendon against coracoacromial arch.
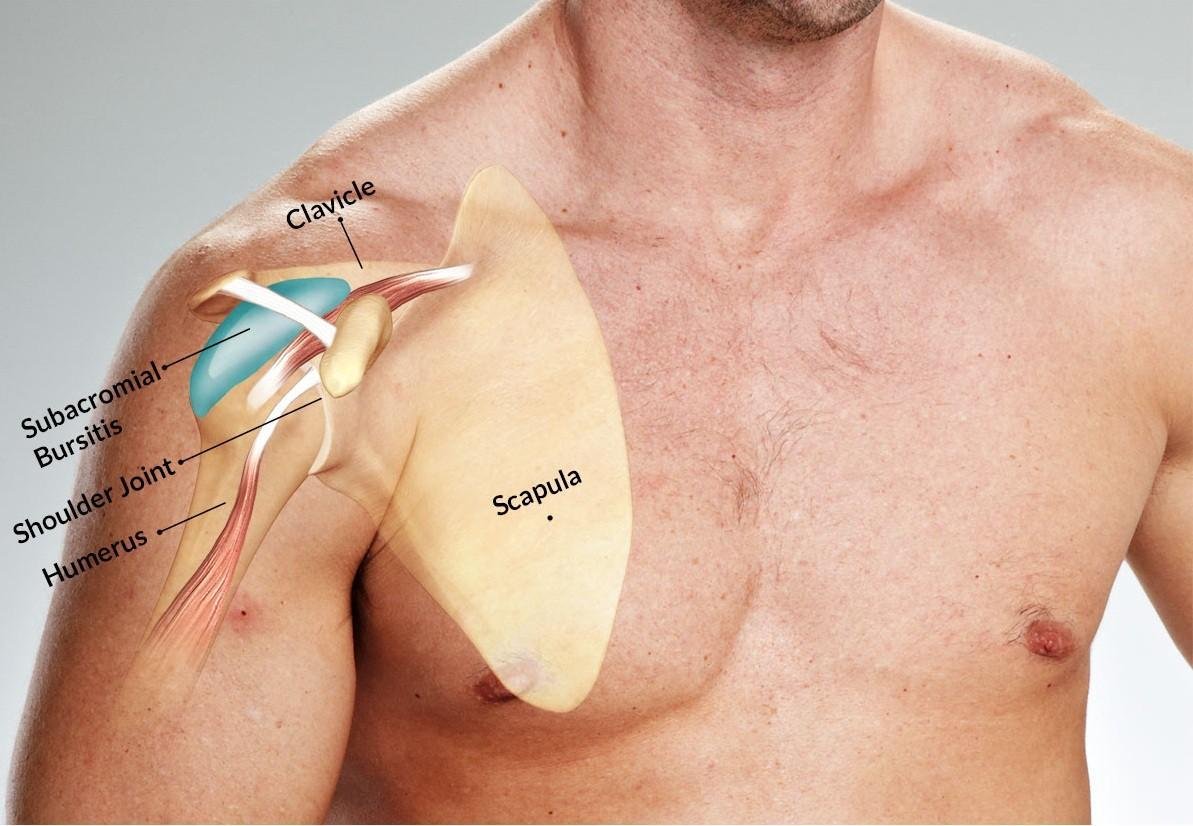
Subacromial buritis
Inflammation of bursa due to deposition of calcium within supraspinatus tendon. It is common in middle aged males. Patient complains of painful movement during abduction from 50°-130°
Popeye’s deformity
Osteoarthritic changes may cause rupture of long head of biceps tendon. Tendon may be avulsed from supraglenoid tubercle of scapula. Detached muscle contracts into a ball in anterior arm on attempted elbow flexion.

Paralysis of trapezius
Trapezius is the only muscle that elevates shoulder. Paralysis from a stroke causes a drooping shoulder and inability to shrug.