Wilms’ tumor is a rare kidney cancer that primarily affects children. Also known as nephroblastoma, it’s the most common cancer of the kidneys in children. Wilms’ tumor most often affects children ages 3 to 4 and becomes much less common after age 5. Wilms’ tumor most often occurs in just one kidney, though it can sometimes be found in both kidneys at the same time.

Epidemiology
- Peak incidence: 2–5 years
- Most common malignant neoplasm of the kidney in children
Etiology
The exact etiology of Wilms tumor remains unknown, but it is associated with several genetic mutations and syndromes.
Genetic predisposition
- Gene mutations have been found in children both with and without genetic syndromes who have Wilms tumor.
- The WT1 (Wilms tumor 1) gene is the most important Wilms tumor gene (mutated in ∼ 10–20% of cases)
Associated syndromes
- Approx. 10% of Wilms tumors occur in children with syndromes.
- Denys-Drash syndrome (point mutation in WT1 gene, which encodes a zinc finger transcription factor)
- Wilms tumor
- Pseudohermaphroditism, undescended testes in males (due to gonadal dysgenesis)
- Early-onset nephrotic syndrome
- WAGR syndrome (deletion of the 11p13 band → deletion of WT1 gene and other genes such as PAX6)
- Wilms tumor
- Aniridia
- Genitourinary (GU) anomalies – Pseudohermaphroditism, undescended testes in males (due to gonadal dysgenesis) and early onset nephrotic syndrome
- Intellectual disability (mental Retardation)
- Beckwith-Wiedemann syndrome (mutations of WT2 gene)
Clinical features
- Abdominal mass (often found incidentally) which is non-tender, unilateral, not crossing midline (however, up to 10% of cases are bilateral and/or multifocal), smooth and firm.
- Other signs and symptoms include
- Abdominal pain (∼ 40% of cases)
- Hematuria (∼ 25% of cases)
- Hypertension (∼ 25% of cases)
- In cases of subcapsular hemorrhage: anemia, and possibly fever
- Symptoms caused by metastatic spread (e.g., pulmonary symptoms)
Diagnosis
- Urinalysis: hematuria may be present
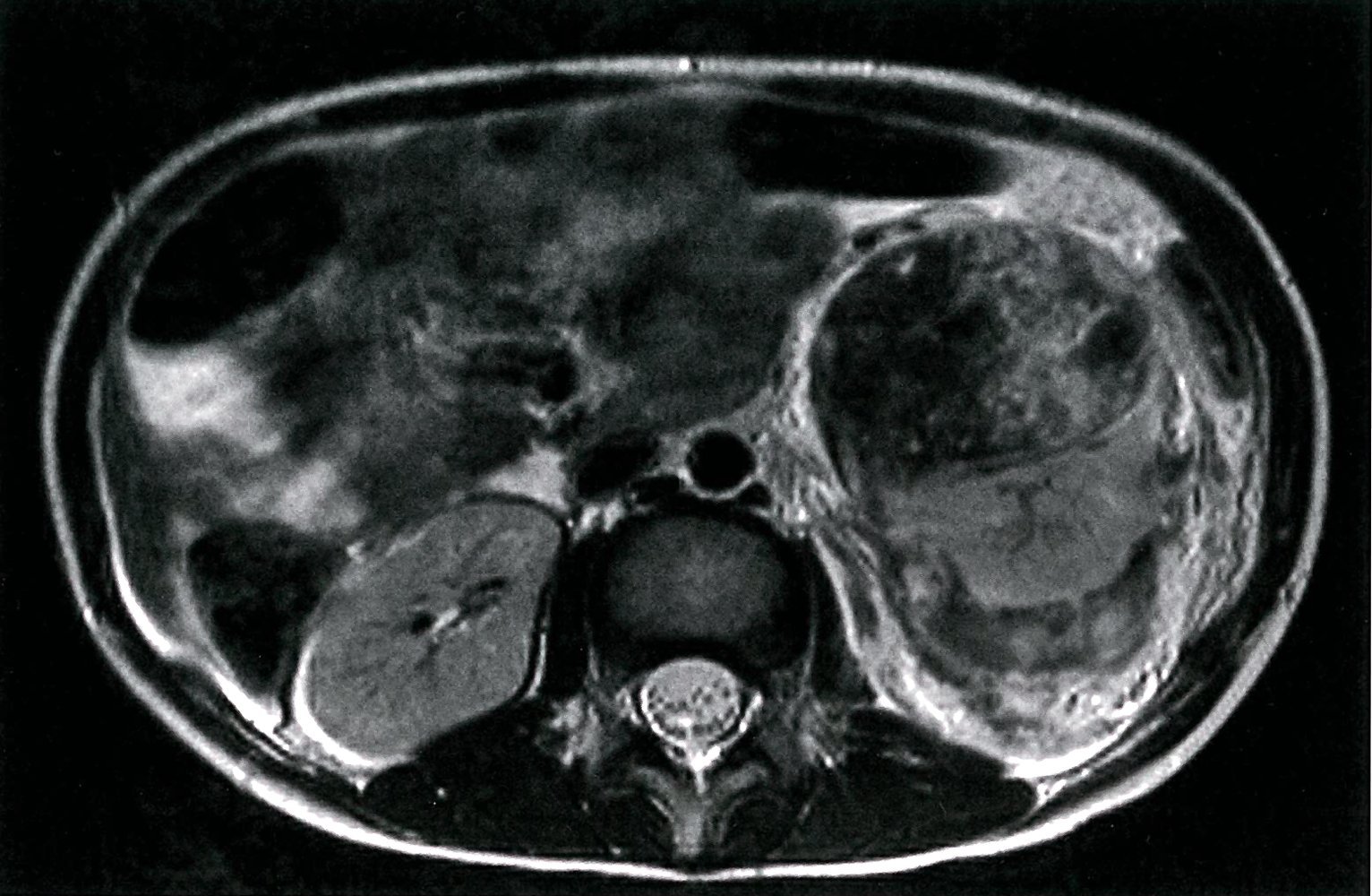
- Imaging
- Best initial test: USG (Hypervascular tumor, mostly uniform echogenicity with hypoechoic areas of necrosis)
- Abdominal CT/MRI: assess extent of involvement and help with surgical planning
- CT thorax/CXR: determine metastases and staging
- Biopsy is usually reserved for assessing nodules

Pathology
Wilms tumor consists of embryonic glomerular structures and may include cysts, hemorrhage, or necrosis. It typically has a pseudocapsule.
Staging

Differential Diagnosis

Treatment