CROHN’S DISEASE
It is a bowel disorder without any certain etiology characterized by transmural inflammation of gastrointestinal tract. It may involve any region from mouth to perianal area.
ETIOLOGY
Age: 15-25 years
No gender predilection
80% of the people have small bowel involvement.

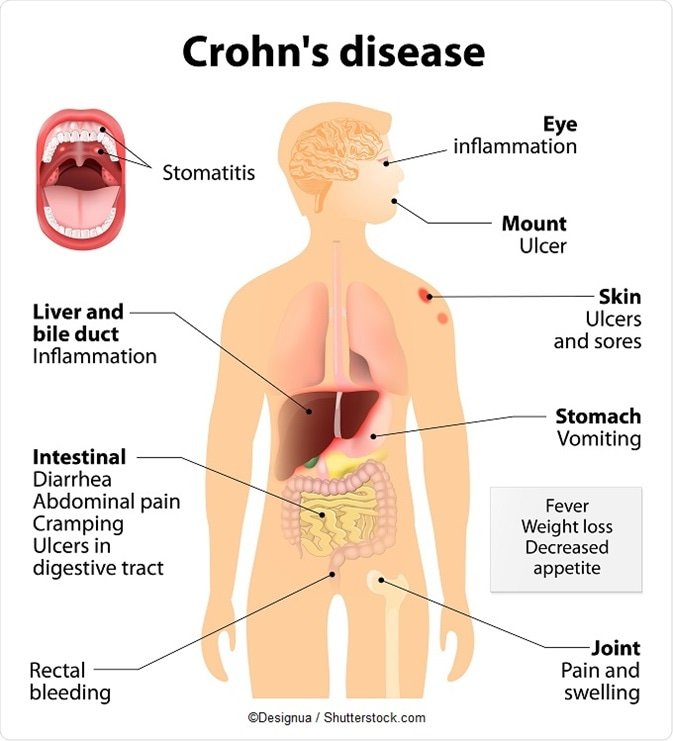
CLINICAL MANIFESTATIONS
Abdominal pain: Frequently right lower quadrant pain, crampy, transmural nature of this disease results in fibrotic structures. These strictures can lead to intestinal obstruction.
Diarrhea: Any H/O prolonged diarrhea without bleeding points towards IBD (Inflammatory Bowel Disease)
Bleeding: presence of microscopic level of blood may be seen, however gross presence is infrequent.
Fistulas: Due to transmural inflammation sinus tracts develop leading to fistulas
Severe oral involvement may be present manifest as aphthous ulcer
Fatigue and weight loss
Extraintestinal
- Arthritis or arthropathy: large joints are mostly involved
- Eyes: in 5% cases uveitis, episcleritis
- Skin: Erythema nodosum and pyoderma gangrenosum
- Primary sclerosing cholangitis
- Renal stones
- Pulmonary: chronic bronchitis, bronchiolitis, sarcoidosis
DIFFERENTIAL DIAGNOSIS
Irritable bowel syndrome
Lactose intolerance
Infectious colitis
Ulcerative colitis
DIAGNOSIS
Physical examination: Pallor, weight loss, perianal skin tags, abdominal tenderness
CBC: Anemia, Iron deficiency, elevated WBC, B12 deficiency, elevated ESR or CRP
Stool specimen
Colonoscopy: Involves terminal ileum usually with skip areas of involvement, Pseudopolyps, Rectal sparing, Granulomas may be noted
Air contrast barium enema may show extent of disease
MRI to detect perianal fistulas
Radio logic imaging
On control films presence of gallstones, renal oxalate stones, and sacroiliac joint or lumbosacral spine changes should be sought
USG shows bowel hyperemia and small bowel wall thickening
Antibody Tests: Antineutrophil cytoplasmic antibodies(pANCA) and anti saccharomyces cerevisiae antibodies(ASCA)
Barium small bowel follow-through include:
mucosal ulcers
aphthous ulcers initially
deep ulcers (>3 mm depth)
longitudinal fissures
when severe leads to cobblestone appearance
may lead to sinus tracts and fistulae
string sign: tubular narrowing due to spasm or stricture depending on the chronicity
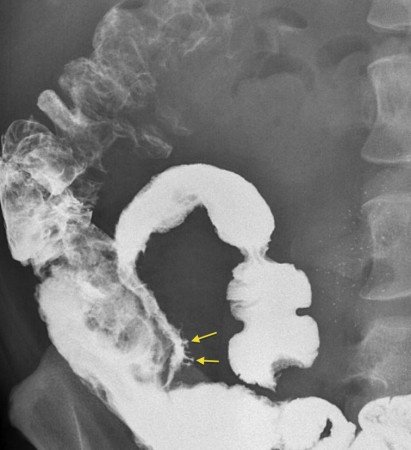
( In this picture the deep, linear ulcers (arrows) that have filled with barium in this stenosed terminal ileum are known as ‘rose-thorn ulcers’ and are typical of Crohn’s disease )
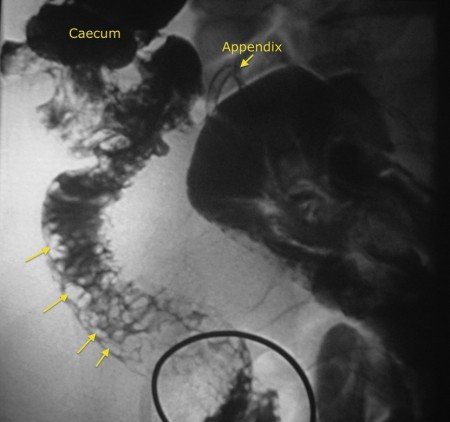
( In this picture it shows the classic appearance of Crohn’s disease in the terminal ileum – so-called ‘cobblestoning’. This is caused by extensive fissures and ulceration in between areas of intact but oedematous mucosa, resembling cobblestones (arrows) )
MANAGEMENT
Management is complex as the condition is chronic with a relapsing-remitting course. Medical management includes corticosteroids, 5-ASA preparations, immunomodulation (e.g. azathioprine, cyclosporine, methotrexate) 7. Surgical management is reserved for complications.
COMPLICATION
Strictures
Adhesions and bowel obstructions
Perianal disease
Fistula
Perianal abscess