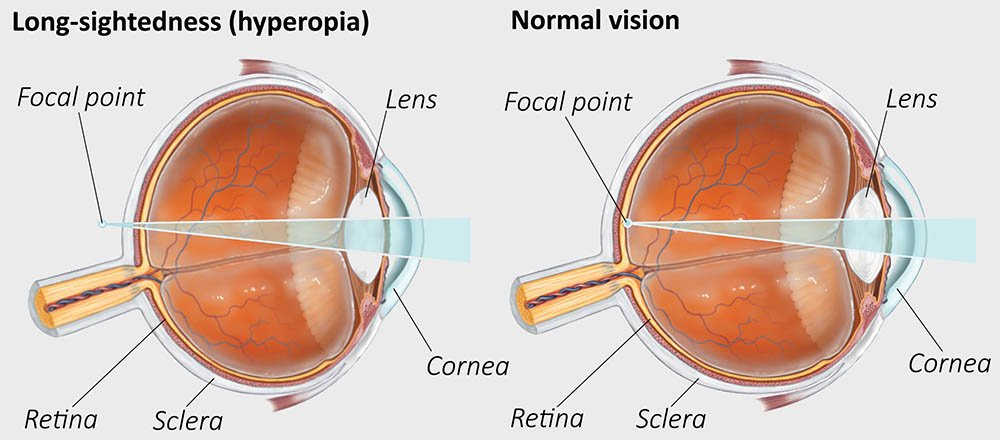
Hypermetropia is the refractive error in which the parallel rays of light coming from infinity are focused behind the retina with accommodation being at rest
- Person cannot see near objects clearly
- Also known as Long sightedness or Hyperopia
Etiology
Physiological types
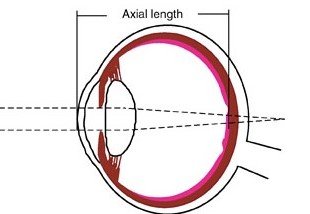
Axial hypermetropia:
- Commonest form
- Due to axial shortening of eyeball
- 1 mm shortening of antero-posterior diameter results in 3 diopters of hypermetropia
- May be developmental or pathological
Curvatural hypermetropia:
- Curvature of cornea, lens or both is flatter than the normal, resulting in decrease in refractive power
- 1mm increase in radius of curvature results in 6 diopters of hypermetropia
- May be developmental or rarely pathological

Index hypermetropia:
- Due to decrease in refractive index of lens in old age due to cortical sclerosis.
- Also in diabetics under treatment
Positional hypermetropia:
- Due to posteriorly placed lens
Absence of crystalline lens:
- Either congenital or acquired
Consecutive hypermetropia due to:
- Overcorrected myopia
- Underpowered IOL implantation
Clinical types
Simple or developmental or physiological hypermetropia:
- Due to biological variations in development of eyeball
- It includes-
- Developmental axial hypermetropia
- Developmental curvatural hypermetropia
Non-physiological hypermetropia:
- Congenital
- Microphthalmos
- Nanophthalmos
- Microcornea
- Congenital lens subluxation
- Congenital aphakia
- Acquired
- Senile hypermetropia ( index type)
- Positional hypermetropia (subluxation of lens)
- Aphakia
- Consecutive (due to overcorrected myopia surgically)
- Pseudo-phakia (due to underpowered IOL implantation)
- Functional hypermetropia:
- Paralysis ( III rd nerve) of accommodation
Nomenclature (components of hypermetropia)
Nomenclature for various components of the hypermetropia is as follows:
Total hypermetropia is the total amount of refractive error, which is estimated after complete cycloplegia with atropine. It consists of latent and manifest hypermetropia –
Latent hypermetropia
- It implies the amount of hypermetropia (about 1D) which is normally corrected by the inherent tone of ciliary muscle.
- The degree of latent hypermetropia is high in children and gradually decreases with age. The latent hypermetropia is disclosed when refraction is carried after abolishing the tone with atropine.
Manifest hypermetropia
It is the remaining portion of total hypermetropia, which is not corrected by the ciliary tone.
- It consists of two components, the facultative and the absolute hypermetropia.
- Facultative hypermetropia constitutes that part which can be corrected by the patient’s accommodative effort
- Absolute hypermetropia is the residual part of manifest hypermetropia which cannot be corrected by the patient’s accommodative efforts.
Total hypermetropia = latent + manifest (facultative + absolute)
Clinical features
Symptoms:
- Blurred vision (more for near than distant)
- Asthenopic symptoms- tiredness of eyes, frontal headache, watering, mild photophobia
Signs:
- Size of eyeball- small
- Cornea- small
- Anterior chamber- shallow
- Ophthalmoscopy-
- Pseudopapillitis (optic disc is smaller, hyperemic)
- Shot silk appearance of retina
- Retinoscopy and Autorefractometry reveals Hypermetropic refractive error
Grading of Hypermetropia
Low Hypermetropia– when error is ≤ 2D
Moderate hypermetropia– error is between +2 to +5D
High hypermetropia– error is ≥ +5D
Complications
- Recurrent styes, blepharitis or chalazia may occur
- Accommodative convergent squint
- Amblyopia
- Predisposition to develop primary narrow angle glaucoma
Treatment
Optical treatment
Basic principle of treatment is to prescribe convex (plus) lenses, so that the light rays are brought to focus on the retina.
Fundamental rules for prescribing glasses in hypermetropia include:
- Total amount of hypermetropia should always be discovered by performing refraction under complete cycloplegia.
- The spherical correction given should be comfortably acceptable to the patient. However, the astigmatism should be fully corrected.
- Gradually increase the spherical correction at 6 months interval till the patient accepts manifest hypermetropia.
- In the presence of accommodative convergent squint, full correction should be given at the first sitting.
- If there is associated amblyopia, full correction with occlusion therapy should be started.
Modes of prescription- Spectacles and Contact lens

Surgical treatment
Corneal based procedures-
- Thermal laser keratoplasty
- Conductive keratoplasty
- Hyperopic PRK
- Hyperopic LASIK
Lens based procedures-
- Phakic refractive lens (PRL) or implantable contact lens (ICL)
- Refractive lens exchange