Septoplasty or alternatively submucous septal resection and septal reconstruction, is a corrective surgical procedure done to straighten a deviated nasal septum – the nasal septum being the partition between the two nasal cavities.

SEPTOPLASTY
Conservative approach to septal surgery; Mucoperichondrial/periosteal flap is raised only on one side; Replaced SMR.
INDICATIONS
- DNS
- As part of Septorhinoplasty
- Recurrent epistaxis from spur
- Sinusitis d/t septal deviation
- Septal deviation causing contact headaches
- For approach to middle meatus or frontal recess in FESS
- Access to endoscopic DCR operation
- Approach to pituitary fossa
- Septal deviation causing sleep apnoea
CONTRAINDICATIONS
- Acute nasal or sinus infection
- Untreated DM
- Hypertension
- Bleeding diathesis
ANAESTHESIA
Local or General
POSITION
Reclining position with head end of table raised.
PROCEDURE
- Septum infiltrated with 1% Lignocaine; Adrenaline 1:1,00,000
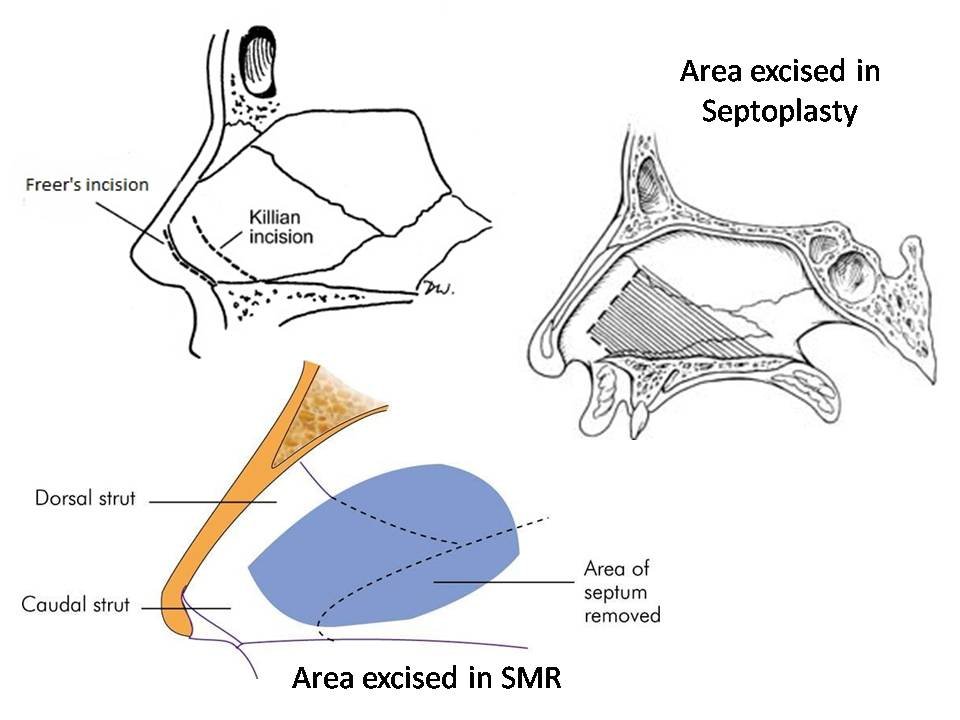
- A slightly curvilinear incision, 2-3 mm above the caudal end of septal cartilage on the concave side (Killian’s incision)
In caudal dislocation- Freer’s incision
- Mucoperichondrial/mucoperiosteal flap raised on one side only
- Septal cartilage separated from the vomer and ethmoid plate and flap raised on opposite side
- Maxillary crest removed to realign septal cartilage
- Bony septum corrected by removing deformed parts in many ways-
- Scoring on the concave side
- Cross-hatching or morselizing
- Shaving
- Wedge excision

Further manipulations may be required
- Trans-septal sutures placed
- Nasal pack
POSTOPERATIVE CARE
- Day-care surgery and pt. can go home if he fully recovers from sedation with no postoperative nausea or bleeding. If OSA present, better if observed overnight.
- Strenuous exercise to be avoided as it may cause bleeding.
- Pack, if kept is removed next day and pt. instructed not to sneeze/blow hard; Secretions to be drawn backwards into throat by snorting rather than blowing nose.
- Saline spray/Steam inhalation after pack removal.
- Xylo-/oxymetazoline drops if stuffy nose.
- Nasal splints (removed 4th/8th day) and gentle suction done.
- Pt. should avoid trauma to nose, wipe nose gently and in no case push nose from one side to another.
POSTOPERATIVE COMPLICATIONS
- Bleeding: If severe, packing required.
- Septal haematoma: Evacuate haematoma and give intranasal packing on both sides.
- Septal abscess: Follows infection of septal haematoma.
- Perforation: When opposite sides of mucous membrane tears.
- Depression of bridge: Usually at supratip area d/t too much removal of cartilage along dorsal border.
- Retraction of columella: Caudal strip of cartilage not preserved.
- Persistence of deviation: Inadequate surgery; requires revision surgery.
- Flapping of nasal septum: Too much septal framework removed; flapping right or left with respiration
- Toxic shock syndrome: Staphylococcal/streptococcal surgery following septal surgery
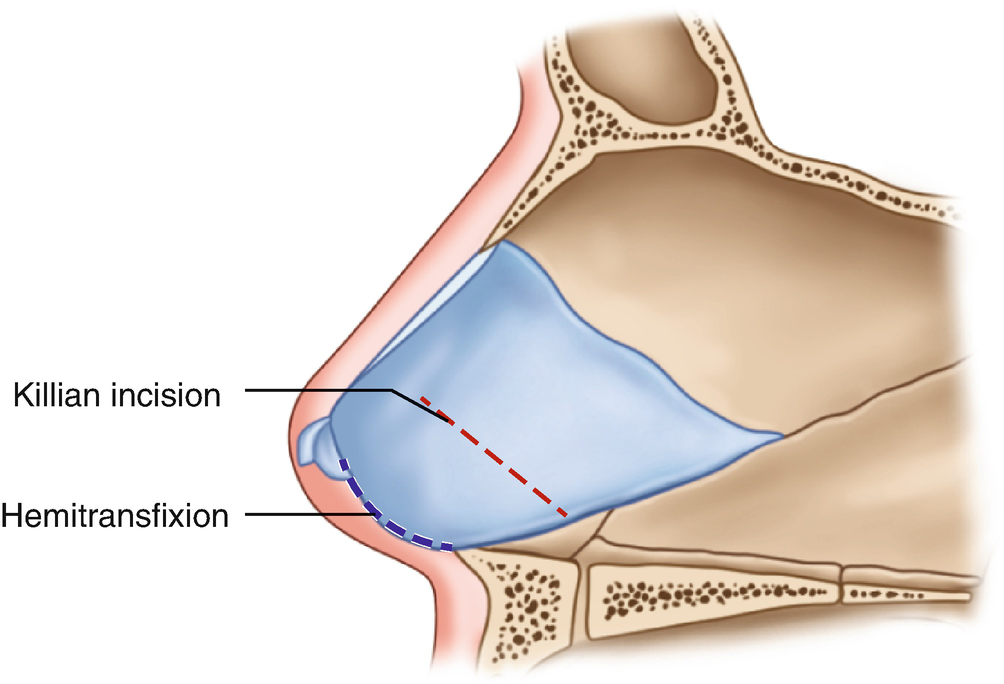
TYPES OF SEPTAL INCISIONS
- Killian’s: In the nasal mucosa, cephalic to the caudal end of the septum
- Transfixion: Through and through incision, close to but caudal to caudal end of the septum.
- Hemitransfixion: Same as the transfixion incision but on one side.
- Horizontal on the spur: For endoscopic spurectomy.
DIFFERENCE BETWEEN SMR AND SEPTOPLASTY
| SMR | Septoplasty |
| Extensive dissection of septum | Limited selective dissection |
| Not done before 17 years | Can be done even in children without affecting nasal growth |
| Flaps raised on both sides of septum | Flaps raised only on one side and limited elevation on the opposite |
| Bony and cartilaginous parts excised | Deformed cartilage is corrected |
| More complications seen | Less complications seen |
| Re-operation difficult | Re-operation easier |