Urine analysis (urinalysis) reflects the state of function of the kidneys and urinary tract. It provides information about metabolic or systemic (nonrenal) disorders. Urine examination should precede all other invasive/noninvasive diagnostic investigations for renal function.
PHYSICAL EXAMINATION
Volume
A healthy adult excretes about 600 to 2000 mL of urine in 24 hours.
Polyuria
Increased urine output which is more than 2 liters in 24 hours.
Causes
• Physiological : Increased fluid intake
• Pathological :
- Diabetes mellitus (polydipsia—excessive intake of water)
- Chronic renal diseases
- Diuretic therapy
- Diabetes insipidus
- Primary aldosteronism.
- Nocturia
- Excretion more than 500 mL of urine at night.
Oliguria
Decreased urinary output which is less than 500 mL in 24 hours.
Causes
• Restricted intake of fluid
• Excessive loss of fluid, e.g. in hemorrhage, burns, dehydration and shock.
• Renal diseases
- Acute glomerulonephritis
- Nephrotic syndrome
- Acute tubular necrosis as in shock, burns, crush syndrome, incompatible blood transfusion and heavy metal poisoning
• Addison’s disease.
Anuria
Markedly diminished urine output, usually less than 125 mL in 24 hours.
Cause
Renal ischemia, tumors and renal stones
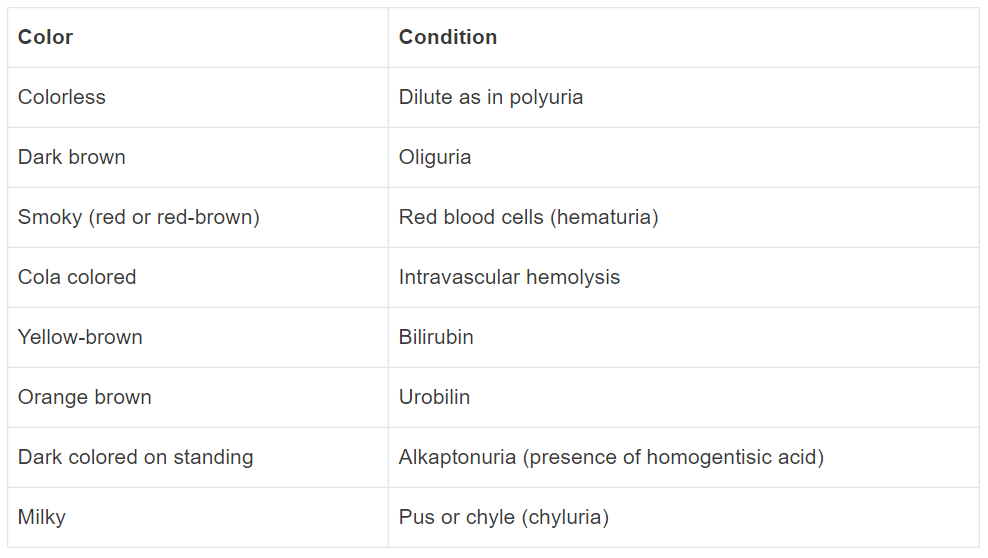
Color
Normal urine is straw to amber colored due to the presence of urochrome pigment, excretion of which is generally proportional to the metabolic rate.
Transparency and Turbidity
Normal urine is usually clear when passed fresh. It may become cloudy, hazy or turbid with the presence of mucus, phosphates, pus, crystals, blood, casts or bacterial growth.
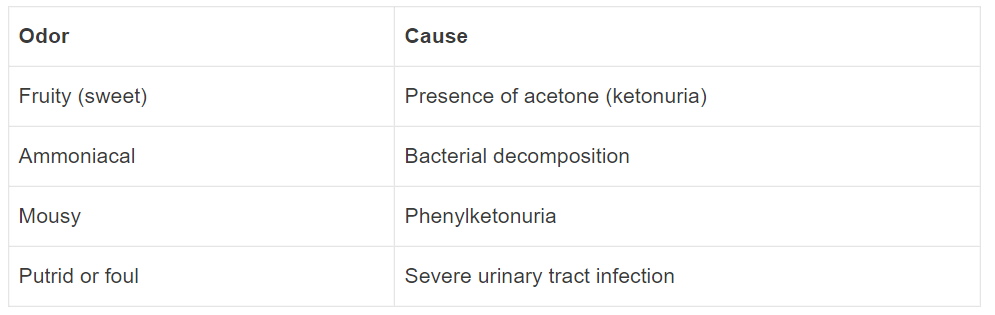
Odor
Normal urine has a faintly aromatic odor because of volatile acids.
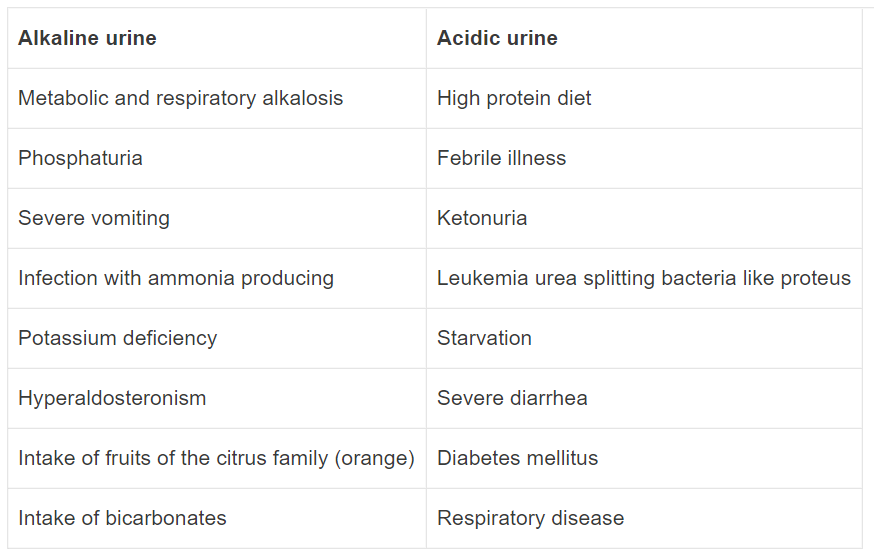
Reaction (pH)
Normal urine is usually acidic with pH varying from 4.6 to 8. Urinary pH is measured as given below.
Specific Gravity
The specific gravity of urine is its density compared with the density of distilled water that is conveniently fixed as 1.000 at 20°C. Normal specific gravity of a 24-hour urine sample is 1.003 to 1.035, average being 1.016.
Specific gravity (SG) is measured by: (1) urinometer, (2) refractometer and, (3) dipstick method.
Increased specific gravity
- Glycosuria
- Dehydration: Restricted fluid intake, diarrhea, vomiting, fever, and excessive sweating.
Decreased specific gravity
- Excessive fluid intake
- Diabetes insipidus
- End stage kidney – Chronic glomerulonephritis, Chronic pyelonephritis, Bilateral polycystic kidneys, Hypertension
Low and fixed specific gravity
When specific gravity is fixed at 1.010, this is known as isosthenuria. It is indicative of severe renal damage (chronic renal failure) with disturbance of both the concentrating and diluting abilities of the kidney.
CHEMICAL EXAMINATION
Proteinuria
The presence of detectable protein in the urine is known as proteinuria. It indicates glomerular injury. If turbid, filter or centrifuge the urine before testing.
Tests for protein
- Heat and acetic acid test
- Sulfosalicylic acid test
- Heller’s test
- Dipstick method
Causes of proteinuria Amount of proteinuria
Glomerular damage
- Nephrotic syndrome Heavy
- Acute glomerulonephritis Mild-to-moderate
- Acute rapidly progressive glomerulonephritis Moderate-to-heavy
- Chronic glomerulonephritis Moderate to Heavy
Tubular damage
- Pyelonephritis Mild
- Acute tubular necrosis Mild
- Polycystic kidney disease Mild
- Heavy metal and vitamin D intoxication Moderate
- Hypokalemia Mild
Prerenal
- Multiple myeloma (Bence Jones protein). Moderate
- Nephrosclerosis Mild-to-moderate
- Malignant hypertension Moderate-to-heavy
- Systemic lupus erythematosus Moderate to Heavy
- Congestive heart failure Mild
- Dehydration Mild
Asymptomatic proteinuria
- After excessive exercise Mild
- Postural (orthostatic) albuminuria Mild
Sugar
These include: glucose, fructose, pentose, galactose, lactose, maltose and sucrose. Special tests are required to differentiate the sugar occurring in urine.
Nonsugar
Ascorbic acid, uric acid, urates, glucuronides, chloroform, formaldehyde, salicylates, streptomycin, phenol, PAS, homogentisic acid (alkaptonuria) and creatinine.
Tests for reducing substance
- Benedict qualitative test
- Dipstick method
Causes of glycosuria
- Diabetes mellitus
- Pregnancy
- Renal glycosuria
- Alimentary glycosuria
- Endocrine disorders
- Acromegaly
- Cushings syndrome
- Hyperadrenocorticism
- Functioning α- or β-cell pancreatic tumors
- Hyperthyroidism
- Pheochromocytoma
- Increased intracranial tension (brain tumor or hemorrhage).
Ketone Bodies
Ketone bodies are three metabolically related compounds:
- Acetoacetic (diacetic) acid
- B-hydroxybutyric acid
- Acetone.
If urine is left at room temperature, acetoacetic acid slowly converts into acetone.
Tests for ketone bodies
- Rothera’s test
- Gerhardt’s test (ferric chloride test)
- Hart’s test
- Dipstick method
Causes of ketonuria
- Diabetic ketoacidosis
- Starvation
- Prolonged vomiting or diarrhea
- Prolonged febrile illness
- Von Gierke’s disease
- Eclampsia
Bilirubin (bile pigment)
Tests for bilirubin in urine provide information concerning metabolic or systemic disorders, especially liver function. Bilirubin is a breakdown product of hemoglobin and is normally not present in urine.
Tests for bilirubin
- Fouchet’s test
- Dipstick methodv
Causes of Bilirubinuria
- Obstructive jaundice: Urine shows bilirubin without urobilinogen
- Hepatocellular jaundice: Bilirubin is absent in urine of patients with hemolytic jaundice.
Urobilinogen
Urobilinogen is normally present in urine in trace amount (1-2 mg/dL) and is insufficient to cause a significant positive reaction.
Tests for urobilinogen
- Ehrlich’s test
- Dipstick method
Causes of Increased Urobilinogen in Urine
- Hemolytic anemias (without bilirubin in urine) – Thalassemia, Sickle cell anemia, Hereditary spherocytosis
- Liver diseases – Preicteric phase of infective hepatitis, Drugs or toxic hepatitis, Cirrhosis.
Bile Salts
Bile salts are composed of mixture of bile acids and glycine or taurine. Two important bile salts are sodium and potassium salts of glycocholates and taurocholates. Normally, bile salts are not present in urine.
Tests for Bile Salts (Hay’s Sulfur Test)
Causes: Hepatocellular and obstructive jaundice
Tests for Blood in Urine
These tests detect hematuria, hemoglobinuria or myoglobinuria.
Hematuria: Presence of red cells in urine, e.g: renal stones, renal cell carcinoma.
Hemoglobinuria: Presence of free hemoglobin in urine, e.g: intravascular hemolysis.
Myoglobinuria: Presence of myoglobin in urine, e.g: crush injury to muscle, strenuous exercise.
Tests for blood
- Benzidine test
- Orthotoluidine test
- Dipstick method
Causes of hematuria
A. Renal diseases
Glomerular causes
- Acute glomerulonephritis
- Renal infarct
- Bacterial endocarditis with kidney involvement
- Malignant hypertension
Nonglomerular causes
- Polycystic kidneys
- Renal cell carcinoma
- Renal stones (nephrolithiasis)
- Trauma (including renal biopsy)
- Renal tuberculosis
- Hydronephrosis
B. Lower urinary tract/prostatic diseases
- Bladder stones (lithiasis)
- Cystitis
- Urethritis
- Carcinoma bladder
- Carcinoma prostate
C. Blood disorders
- Bleeding disorders: Coagulation disorders, severe thrombocytopenia
- Acute leukemia
- Sickle cell disease
D. Miscellaneous
Instrumentation of urinary tract
Causes of hemoglobinuria
- Paroxysmal nocturnal hemoglobinuria (PNH)
- Paroxysmal cold hemoglobinuria (PCH)
- Incompatible blood transfusion
- Severe burns
- Autoimmune hemolytic anemia (AIHA), march hemoglobinuria
- Snake bite
- Blackwater fever (falciparum malaria)
MICROSCOPIC EXAMINATION
Cells: They are expressed as number of cells per low power or high power field.
- Red blood cells (RBCs)
- White blood cells (WBCs)
- Epithelial cells
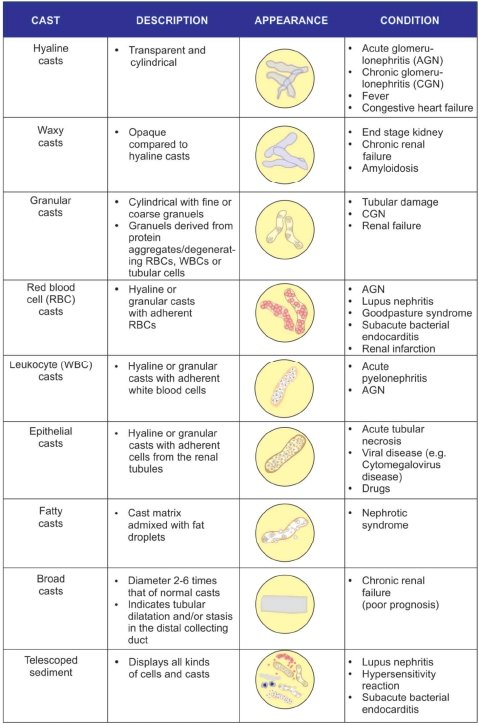
Casts: They are one of the organized elements which are formed only in the kidney and are indicative of a renal disease.
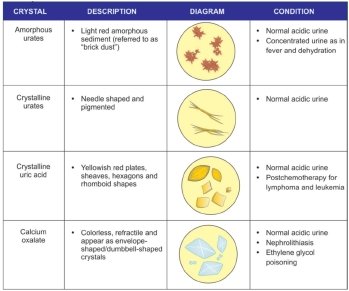
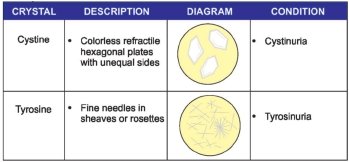
Crystals:
- Crystals in acidic urine
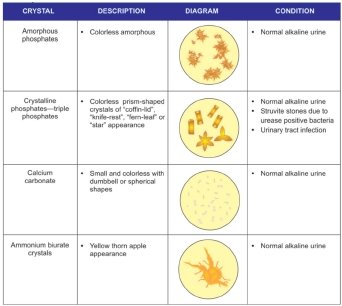
- Crystals found in alkaline urine
- Crystals found in abnormal urine
Others: Abnormal cells and other formed elements
- Malignant cells: Malignant cells exfoliated may be found in malignancies of kidney and bladder.
- Fungi: Yeasts (commonly Candida species) are seen in immunosuppressed patients, like diabetics and patients on cytotoxic drugs.
- Parasites: Parasites that may be found in urine are Trichomonas, Entamoeba histolytica, ova of Schistosoma hematobium and microfilaria.
- Spermatozoa: Sometimes sperms may be normally present and are easily recognized by their structure and motility.
#Know more about Pathology of renal system from “THIS LINK“.
#We Partnered with Achievable.me. Check out their website for awesome study content.