CSOM
Chronic suppurative otitis media (CSOM) is one of the most common childhood infectious diseases worldwide and is a common cause of hearing impairment in resource-limited settingsIt is characterized by chronic drainage from the middle ear associated with tympanic membrane perforation CSOM is usually preceded by an episode of acute otitis media (AOM).
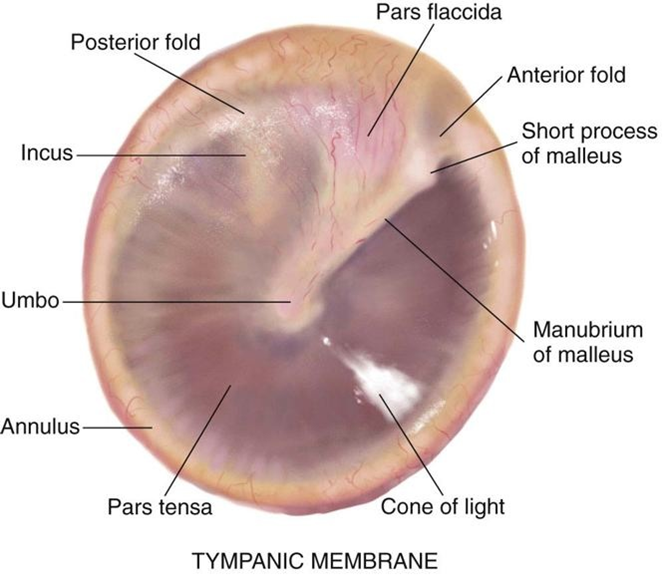
Normal ear anatomy
World Health Organization (WHO) defines CSOM as ≥ 2 weeks of otorrhea. Generally, patients with tympanic membrane perforations and discharge persisting from 6 weeks to 3 months, despite medical treatment, are diagnosed with CSOM.
Types
CSOM is classified into 2 main types
Attico-antral type (attic or marginal perforation)
- Involves the pars flacida or posterosuperior marginal quadrant.
- Also called “unsafe” type due to potential for dangerous intracranial complications, most commonly caused by cholesteatoma.
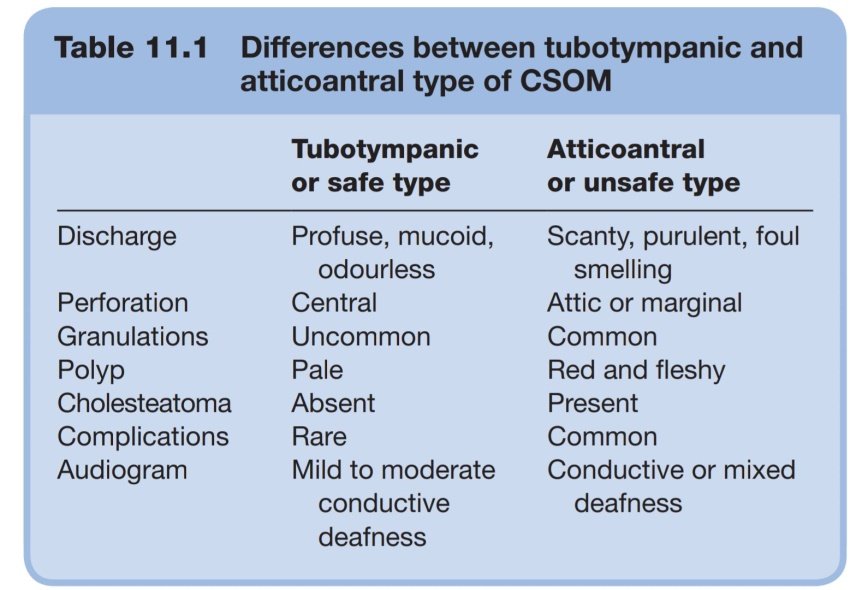
- Discharge usually scanty and malodorous.
- May have moderate to severe hearing loss, potentially resulting in permanent deafness.

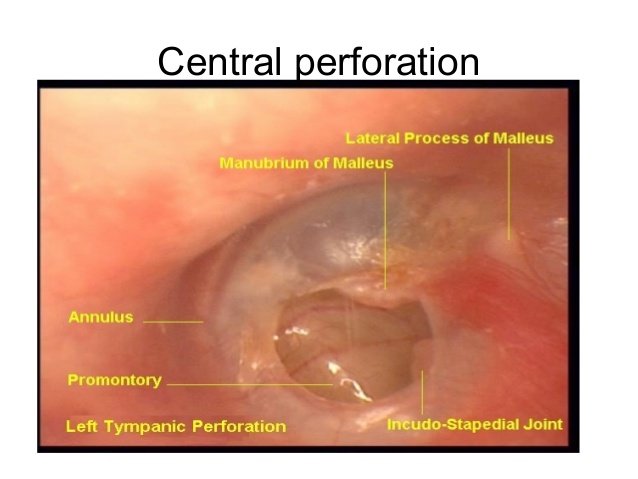
Tubo-tympanic (mucosal) type (central tympanic perforation)
- Involves the pars tensa.
- Also called “safe” type as less likely to result in serious intracranial complications (such as meningitis and brain abscess) compared with attico-antral type.
- Discharge is mainly mucoid or mucopurulent and intermittent.
- Often associated with respiratory tract infection.
- May have mild hearing loss.
Differences
Risk factors
- Low socioeconomic status
- Prolonged symptom duration before seeking medical attention
- Cholesteatoma
- Infection caused by multidrug resistant bacteria
- Underlying HIV infection
Differential Diagnosis
- Bacteremia
- Cholesteatoma
- Hearing Impairment
- Pediatric Nasal Polyps
- Otitis Externa
- Pediatric Bacterial Meningitis
- Rhinovirus (RV) Infection (Common Cold)
Diagnosis is usually based on clinical examination and history.
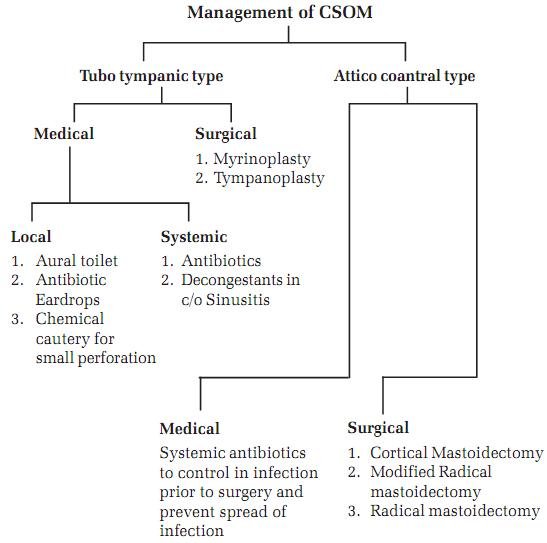
Treatment
Initial Therapy
Aural toilet plus empiric topical antibiotics for initial therapy. The primary goal of treatment is eradicating infection and preventing complications, which is achieved by producing a dry ear.
Educating caregivers on the proper administration of topical antibiotics and other measures that reduce recurrence is an important aspect of initial management.
Aural toilet is a key component of treatment, since it allows the topical antibiotic or antiseptic to truly penetrate to the source of the disease.
Aural toilet is performed until the ear is consistently dry and free of debris.
Ototopical antibiotics — Ofloxacin otic solution (five drops three times a day) or Ciprofloxacin otic solution (0.25 mL single dose container twice daily) for two weeks in addition to aural toilet.
Treatment with topical antibiotic therapy is given with systemic antibiotic therapy for the following reasons:
- Oral antibiotics may have limited efficacy in some patients with CSOM because of tissue damage, inflammation, scarring, and limited vascularization of the middle ear mucosa.
- Systemic side effects are minimized with topical antibiotic therapy, particularly in children .
Fluoroquinolones (eg, ciprofloxacin, ofloxacin) are effective against many of the gram-positive and gram-negative organisms that cause CSOM and are the most commonly used topical medication for CSOM
Ototopical corticosteroids — Topical corticosteroid use (usually in combination with an ototopical antibiotic) is controversial and not well studied. only use a combination drop (antibiotic plus corticosteroid) if granulation tissue
Antiseptic agents — Use of topical antiseptic agents to clean the ear canal and middle ear of debris is generally limited to settings where suction is unavailable.
Complications
Infectious extra- and intracranial complications — Extra- and intracranial complications occur when the infection spreads through natural or pathologic bony dehiscences and vascular channels to involve the mastoid, facial nerve, labyrinth, lateral sinus, cerebrospinal fluid, and brain.
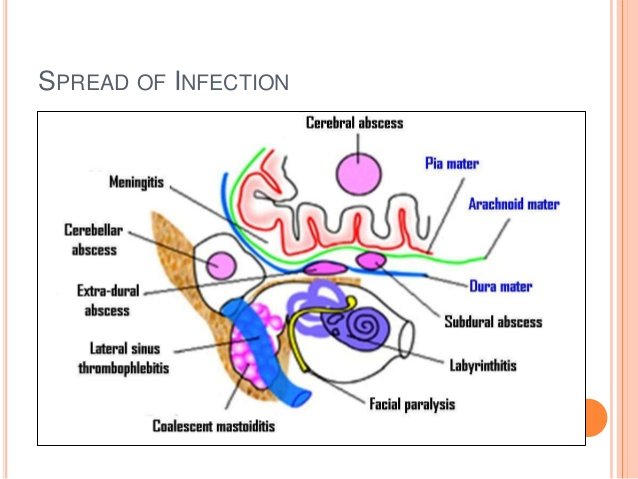
Extracranial complications:
- Mastoiditis
- Subperiosteal abscess: Subperiosteal mastoid abscesses are often associated with cholesteatoma
- Facial paralysis : facial nerve palsy suggests inflammation of the facial nerve
- Labyrinthitis :Dizziness suggests a labyrinthine fistula.
Intracranial complications:
- Patients with intracranial complications often present with fever, headache, earache, vestibular symptoms, meningeal signs, and alteration in mental status
- Meningitis
- Subdural, epidural, perisinus, or brain abscess
- Lateral sinus
Brain abscess and meningitis are the most commonly reported intracranial complications.
Extracranial and intracranial complications often necessitate surgery in addition to broad spectrum intravenous antibiotics.
Reference: ENT dhingra, Uptodate medscape



Very Well written ♥️
Thank you for your valuable contact..