Patients with atrial fibrillation, even when it is paroxysmal or occurs rarely, the need for oral anticoagulation should be evaluated and treatment initiated for those without strong contraindication.
Patients with lone atrial fibrillation (eg, no evidence of associated heart disease, hypertension, atherosclerotic vascular disease, diabetes mellitus, or history of stroke or TIA) under age 65 years need no antithrombotic treatment.
Patients with transient atrial fibrillation, such as in the setting of acute MI or pneumonia, but no prior history of arrhythmia, are at high risk for future development of atrial fibrillation and appropriate anticoagulation should be initiated based on risk factors.
In reversible cause, such as after coronary artery bypass surgery or associated with hyperthyroidism, then long-term anticoagulation is not necessary.
CHADS2 Risk Score consist of Cardiac failure, Hypertension, Age ≥ 75 years, Diabetes, Stroke. In addition to the traditional five risk factors, the European and American guidelines recommend that three additional factors included in the CHA2DS2-VASc score be considered presence of Vascular disease, Age 65–74 years and Female Sex.
CHA2DS2-VASc Risk Score for assessing risk of stroke and for selecting antithrombotic therapy for patients with atrial fibrillation:

The CHA2DS2-VASc score is especially relevant for patients who have a CHADS2 score of 0 or 1
CHA2DS2-VASc score ≥ 2, oral anticoagulation is recommended
CHA2DS2-VASc score = 1, oral anticoagulation should be considered, taking into account risk, benefit, and patient preferences.
Unfortunately, studies show that only about half of patients with atrial fibrillation and an indication for oral anticoagulation are receiving it, and even when treated with warfarin, they are out of the target INR range nearly half the time.
One reason for undertreatment is the misperception that aspirin is useful for prevention of stroke due to atrial fibrillation. In the 2016 European guidelines, aspirin is given a class III A recommendation, indicating that it should not be used because of harm (and with no good evidence of benefit).
Cardioversion should be performed after at least 3–4 weeks of anticoagulation at a therapeutic level.
Anticoagulation clinics with systematic management of warfarin dosing and adjustment have been shown to result in better maintenance of target anticoagulation.
Four Direct oral anticoagulants (DOACs) or New oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, and edoxaban – have been approved by the FDA for stroke prevention in patients with atrial fibrillation.
(These medications have not been studied in patients with moderate or severe mitral stenosis, and they should not be used for patients with mechanical prosthetic valves. The term “nonvalvular atrial fibrillation” is no longer used in the European guidelines since most patients with other types of valvular heart disease have been included in trials of DOACs, which are equally effective in these patients.)
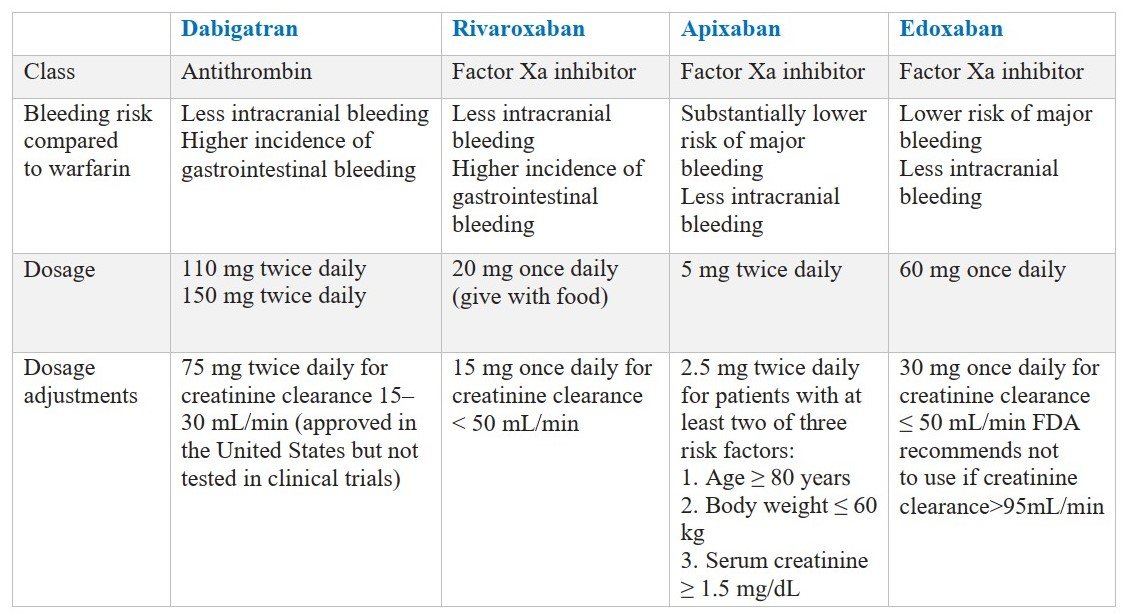
These four DOACs have important advantages over warfarin, and therefore they are recommended preferentially over VKAs.
DOACs are safe and effective for patients with moderate or severe valvular abnormalities, with the exception of moderate or severe mitral stenosis.
For lower rates of intracerebral hemorrhage, DOACs advantage over warfarin in the elderly and the frail, including patients with history of falls.
Some patients with atrial fibrillation should be treated with VKAs, those are:
- Who have mechanical prosthetic valves
- Advanced kidney disease (creatinine clearance less than 25 mL/min)
- Moderate or severe mitral stenosis
- Who cannot afford the newer medications.
Stable patient who receiving warfarin for a long time, with a high time in target INR range, and who are at lower risk for intracranial hemorrhage will have relatively less benefit with a switch to a newer medication.
Important issues with using the DOACs:
- Important to monitor kidney function at baseline and at least once a year, or more often for those with impaired kidney function.
- Each of the medications interacts with other medications affecting the P-glycoprotein pathway, like oral ketoconazole, verapamil, dronederone and phenytoin.
- Each of the medications has a half-life of about 10–12 hours for patients with normal kidney function.
- For elective procedures, stop the medications two to three half-lives (usually 24–48 hours) before procedures with low to moderate bleeding risk (ie, colonoscopy, dental extraction, cardiac catheterization), and five half-lives before procedures like major surgery.
- Discontinuation times should be extended in patients with impaired renal function, particularly with dabigatran.
There are no practical tests to immediately measure the effect of the medications, although a normal aPTT suggests little effect with dabigatran, and a normal prothrombin suggests little effect with rivaroxaban.
If bleeding occurs standard measures like, diagnosing and controlling the source, stopping antithrombotic agents and replacing blood products should be taken. Use activated oral charcoal if the patient taken DOACs in the prior 2–4 hours to reduce absorption and if the patient is taking aspirin, consider platelet transfusion.
Patient with severe bleeding while taking dabigatran may be treated with the reversal agent idarucizumab, which is a humanized monoclonal antibody approved by the FDA for rapid reversal of the anticoagulation effects, for use in the event of severe bleeding or the need for an urgent procedure. Andexanet alfa, an intravenous factor Xa decoy, is approved for reversal of factor Xa inhibitors.
Aspirin should not be used with the DOACs unless there is a clear indication, such as acute coronary syndrome within the prior year. (Like with warfarin, there appears to be a 1.5- to 2-fold increased rate of bleeding associated with the use of aspirin in combination with the DOACs.)





this platform is very informative for students ,thanks Ashis rong sir for suggesting me this app
Welcome to Medical Junction family. Thanks for the support. You can help us by sharing this app with your friends.