Acute post streptococcal glomerulonephritis is an immunologic response of the kidney to infection, characterized by the sudden appearance of edema, hematuria, proteinuria and hypertension . It is essentially a disease of childhood that accounts for approximately 90% of renal disorders in children.
Causative organism
Group A beta hemolytic Streptococcus ( Strains M1, M4, M12)
Pathogeneses
Molecular Mimicry– Antibodies against streptococcal antigens react with normal glomerular antigens leading to immune complex formation & complement activation. Release of leukocyte, macrophage, cytokines further increases injury.
Clinical Features
- Age- School age children , uncommon below 3 years
- Gender- More common in boys
- Subclinical episodes are more common than overt disease especially during epidemics
- Onset is rapid with puffiness around eyes and pedal edema.
- Cola colored wine lasts for few hours to few days.
- Hypertension – Patients should be monitored for symptoms of encephalopathy like blurred vision, headache, seizures etc.
- Acute phase resolves in 6-8 weeks

Pathology
Light Microscopy– Enlarged and ischemic glomeruli, capillary loops narrowed with mesangial cell proliferation and neutrophil infiltration.

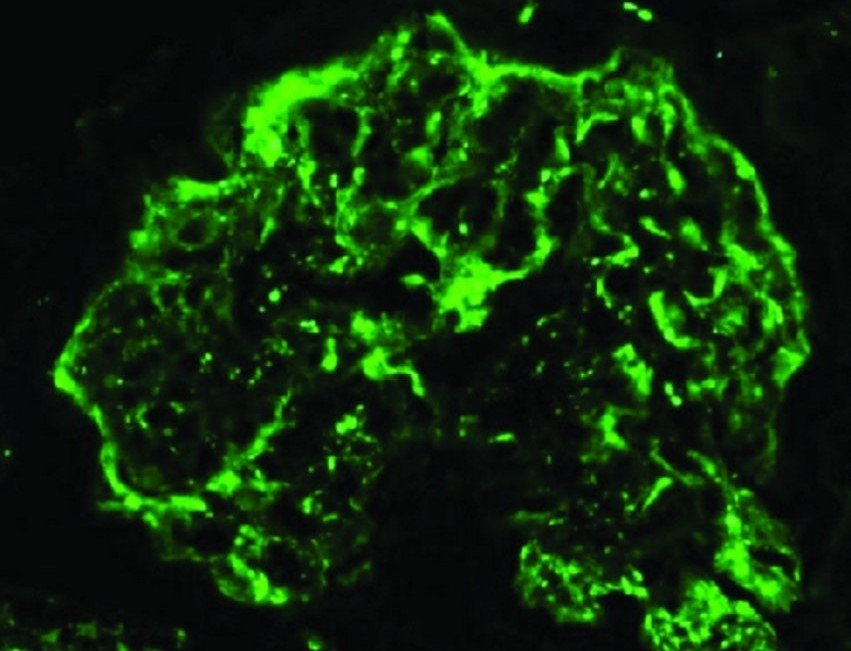
Immunofluorescence– Granular deposits of lgG and complement along capillary wall ( ‘Lumpy-Bumpy’ deposits ).
Election Microscopy– Deposits (humps) on sub epithelial side of glomerular basement membrane & in mesangium.

Laboratory Findings
- Urine Analysis– Dysmorphic RBC, Polymorphonuclear leukocytes, RBC cast, Proteinuria 1-2 +
- Increased Blood urea and creatinine
- Hyponatremia, Hyperkalemia, Metabolic acidosis
- Normocytic anemia, Raised ESR, Low grade hemolysis
- Low (3 levels which normalizes by 8-12 weeks
- Evidence of prior streptococcal infection– ↑ASO titers ( 80% ) or anti-DNase B (skin infection )
- Chest X-ray – Prominent bronchovascular marking indicating hypervolemia
Treatment
- Mild oliguria with normal BP can be managed at home
- Diet–
- Sodium, potassium and fluid restriction till blood levels of creatine reduce and wine output increases.
- Prevent overhydration as it can precipitate left ventricular failure
- Diuretics–
- Modest edema = Oral frusemide ( 1-3mg/ kg)
- Pulmonary edema-IV frusemide (2-4 mg/kg)
- Daily weight and wine output monitoring
- Hypertension –
- Mild – Fluid and salt restriction
- Antihypertensive include Amlodipine, Nifedipine
- Hypertensive emergency – IV Nitroprusside & Labetalol
- Left Ventricular Failure – Control Hypertension and induce diuresis by IV frusemide. If no diuresis noted start dialysis
- Dialysis–
- Severe renal failure
- Prolonged oliguria
- Fluid overload
- Life threatening electrolyte disturbance
- Penicillin given if active pharyngitis or pyoderma is present





These are great notes.I found it very useful
Thanks to our author. We’ll be very much helpful if you share our android app with your friends. Have a nice day. 😊
I’m glad you found them useful!